
MS Increases with Distance from the Equator: Examining the Latitude Gradient
Part 3 of the Neuroepidemiology series.

Multiple sclerosis (MS) is an autoimmune disease that results in damage, in the form of lesions, to the insulating structures of nerve cells in the brain and spinal cord. With a largely unknown cause, it has has long been thought to be a multifactorial, complex disorder that is both genetically and environmentally determined. One of the most striking neuroepidemiological observations is that the prevalence of MS increases with distance from the equator. That is, populations living at higher latitudes have more cases of MS than those living nearer the equator. In this blog post I review the evidence for the latitude gradient in MS prevalence while exploring the underlying mechanisms, in particular the role of ultraviolet (UV) exposure and the synthesis of vitamin D, and discuss what I believe to be an important confounder: variations in access to healthcare. And lastly, I’ll briefly refer to other environmental risk factors further shaping the landscape of MS.
Introduction
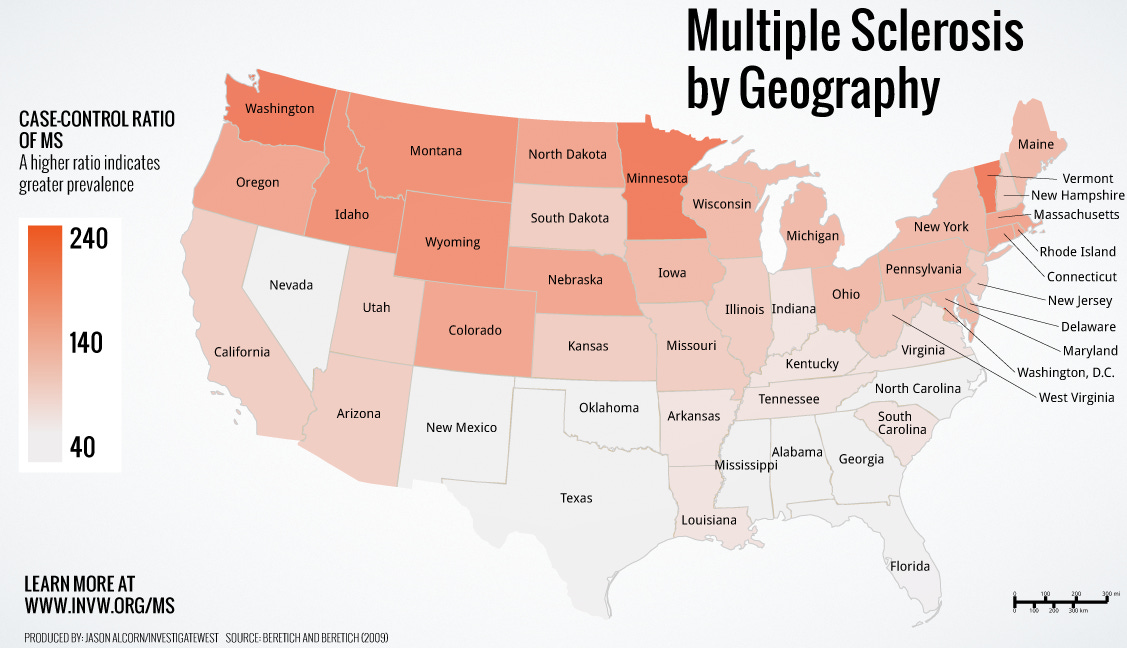
The suggestion that "MS increases with distance from the equator" is a fascinating one. Several studies have shown that individuals in higher latitude positions are statistically more prone to having MS than individuals at closer-to-equator residences [1]. This gradient, or trend of latitude, has been noted across various continents, from Europe and Latin America to North America and Australia.
What is striking here is while MS is affected by an abundance of environmental as well as hereditary factors, the limelight of the current moment focuses on the gradient of latitude and perhaps what its mechanisms might be. By recognizing the function of UV exposure and vitamin D, along with the constraint imposed by underdiagnosis in lower latitude countries with weaker healthcare infrastructure, we can start to untangle why geography seems to play a role in MS risk. We will also briefly position the latitude gradient within other environmental etiologies, so that our emphasis on latitude is well-supported and situated within the context of the wide range of risk factors.
The Latitude Gradient in MS Prevalence
The latitude gradient is a proven fact: the farther away from the equator, the higher the prevalence of MS. This has been quantified in numerous studies to rise by around 5-6 cases per 100,000 people per degree of latitude from the equator [2][3]. This has been replicated repeatedly in different populations and geographical settings.
For instance, prevalence surveys conducted in Latin America, Europe, and Australia indicate that the higher latitude areas have far greater MS prevalence than equatorial regions [1][2]. The correlation exists even after adjusting for population age structure variation, suggesting that the gradient cannot be a demographic variation artifact. Notably, though prevalence data reflect a cumulative overview of disease burden, incidence studies, which monitor the onset of new cases, have been more inconsistent, partially because of disparity in access to healthcare and patterns of diagnosis (a point that we will be revisiting shortly).
Mechanisms Underlying the Latitude Gradient
The most prominent mechanism proposed to generate the latitude gradient is variation in the exposure to ultraviolet (UV), and the impacts on the synthesis of vitamin D in the skin. Vitamin D, in addition to its established role in bone physiology, plays a central part in the regulation of immune function. Optimal vitamin D status appears to help control the immune system, and this could be reducing the risk of autoimmune disease such as MS.
UV Exposure and Vitamin D Synthesis
There are greater intensities of UV radiation at tropical latitudes, particularly during winter. High UV exposure means that individuals at these latitudes have higher serum levels of vitamin D. Epidemiological evidence has repeatedly shown a negative correlation between vitamin D and MS risk: as vitamin D decreases, MS risk increases [4]. This relationship is supported by cross-sectional and longitudinal study evidence, as well as by migration studies showing that individuals who migrate from low- to high-latitude regions (or the reverse) adopt the MS risk pattern of their destination, with this being the most pronounced if the move occurs early in life.
Vitamin D's effects on immune modulation are thought to be one of the main reasons for this relationship. It modulates the expression of numerous immune-regulating genes and has the potential to impact the activity of T cells, which are central to the autoimmune process in MS. The reduced capacity for vitamin D production at higher latitudes thus provides a plausible biological rationale for the observed gradient in MS prevalence.
Early-Life Environmental Exposures
The other aspect to consider is that the impact of latitude may be most pronounced during early life. In certain studies, it has been found that risk associated with low vitamin D is highest when the exposure is in utero or in childhood. This suggests that early-life environmental conditions may predispose people to immune system development and later MS risk [5]. If an individual is vitamin D deficient during pivotal immune maturation periods, their susceptibility to MS later in life seems to be increased.
Other Contributing Mechanisms
While the central hypothesis is that of vitamin D deficiency, there may be other mechanisms underlying the latitude gradient. One is genetic predisposition, for instance, which has a major role in risk in MS. Certain genetic influences, such as the HLA-DRB1*15:01 allele, are more prevalent in European populations, who reside predominantly in higher latitude regions [6]. Although this genetic predisposition may mask the relationship between latitude and MS, it cannot fully account for the gradient. Environmental influences, particularly vitamin D deficiency due to reduced UV exposure, remain dominant.
Confounding Factors: The Role of Healthcare Access
One important factor that needs to be considered with utmost caution is the confounding effect of access to healthcare on reported MS incidence and prevalence by latitude. It is plainly obvious that diagnostic facilities and healthcare infrastructure are highly heterogeneous across geographic locations. In several regions near the equator, especially in the developing world, restricted access to healthcare facilities may result in the under or misdiagnosis of MS. This underreporting implies that actual MS incidence in these regions might be higher than reported.
For instance, urban areas such as Bogotá, which is close to the equator but at a high altitude (and thus with high UV exposure), have traditionally had lower MS incidence. But as healthcare services in these areas become better and more accessible, incidence has started to increase, although not to the level of high latitude nations. These results suggest that part of the protective effect of lower latitudes might be explained away to some extent by a lack of diagnostic infrastructure instead of a genuine reduction in risk [7]. If healthcare access is considered, the gradient might be less steep than what studies of prevalence would suggest. In analyzing data for the latitude gradient, investigators must guard against and be mindful of the fact that improvement in diagnostic acumen may reveal an increased underlying incidence of MS in low-latitude areas compared with previously determined rates, which may or may not be cause for alarm.
Background for the Latitude Gradient in Broader Environmental Causes
Although the focus of this post is the latitude gradient, it should be pointed out that MS is caused by a constellation of environmental determinants. Several other environmental causes have been put forward in the cause of MS:
• Viral infections: Epstein–Barr Virus (EBV) is probably the best-established example, and there is a high level of evidence to show that EBV infection increases MS risk [8]. This is an interesting one, given 95-98% of people tested have had an EBV infection at some point, it would seem MS rates should be higher. But , it seems that an infection in adolescence or young adulthood carries a higher MS risk than childhood infection, so it simply isn’t “have you been infected by EBV?” but more “when were you infected”. Other viruses, including Human Herpesvirus 6 (HHV-6), have also been investigated, though their roles are less well understood.
• Lifestyle Factors: Smoking is a known risk factor that not only predisposes towards MS but possibly also worsens its course. Obesity during childhood and young adulthood have been connected with a higher risk of MS because of the connection to long-standing systemic inflammation [9].
• Environmental Toxins: Organic solvent exposure and air pollution have been linked with MS risk, potentially through immune modulation and interaction with genetic processes.
• Circadian Disruption and Stress: Circadian rhythm disruptions—e.g., those experienced by night shift workers—and chronic stress could also contribute to immune dysregulation and increased MS susceptibility.
By setting this latitude gradient within the broader context, we can observe that whilst the geographical pattern is remarkable, it is one component of the multifactorial etiology of MS. Understanding these interactions serves to highlight the requirement for integrated strategies when dealing with prevention and treatment.
Conclusion
The observation that MS prevalence increases with increasing distance from the equator is a robust one that has been consistently demonstrated in numerous studies and populations. Essentially, the latitude gradient is probably driven by differences in UV exposure and its consequent impact on vitamin D synthesis. Lower vitamin D, particularly at times of vulnerability during early life, seems to leave an individual more susceptible to MS, most likely due to its role in modulating the immune system.
The story is not quite so straightforward. In my opinion, an important confounding factor is regional heterogeneity in the availability of health care. Under diagnosis due to lack of access to specializing medical facilities may in many low-latitude regions suppress the incidence of MS. The perceived protective role of low latitudes can lose some of its significance as diagnosis becomes better with time, e.g., as in Bogotá. Because of this, my "Bayesian-ish" interpretation after having learned all this would be that somewhere between 1-2.5/100k cases are simply not being detected within their healthcare systems, leaving an effect of an increase of 2.5-4 cases per 100k people, per degree of latitude. I say this because even studies that attempt to control for healthcare access certainly still have residual confounding. This is because the related variable to control for would be "healthcare access relevant to obtaining a MS diagnosis (eg. neurologists, movement disorder specialists, auto-immune specialists)" as opposed to merely "number of hospitals within X miles" which is the easier, more standard control for these types of studies. My reading emphasizes that one needs to take epidemiological findings with a grain of salt and acknowledge that the latitude gradient, as attractive as it is, isn't the sole risk predictor of MS.
From the larger picture, the latitude gradient remains part of a puzzle too large to get the overall view of. Infectious viruses (particularly EBV), lifestyle factors such as smoking and overweight, environmental toxins exposure from outside, and also circadian disturbance are all risk factors of MS. In terms of understanding MS etiology, all these pieces must be considered while they interact with each other, without isolating any single element.
Although interventions like vitamin D supplementation have been suggested as possible means of reducing the risk increase at higher latitudes, it is important to have realistic expectations. No intervention is likely to be a panacea for MS. Rather, public health measures need to be multi-faceted, addressing a variety of modifiable risk factors and taking into account the underlying genetic predispositions that differ between populations.
Ultimately, further research is required. Future research, particularly that increases diagnostic potential in resource-poor settings and that integrates environmental, genetic, and epigenetic data, will continue to clarify the complex relationship between geography and MS risk. Such insights may lead to more effective prevention strategies, reducing the worldwide burden of MS.
In summary, the latitude gradient in MS prevalence is a strong example of how environmental pressures, specifically exposure to UV radiation and vitamin D status, interact with human biology. As with much epidemiology, however, the association is one that is tempered by concerns about confoundng in the form of access to healthcare and more general environmental factors. By placing the gradient of latitude in context, we not only validate its existence but also present the foundation of a more integrated method of comprehension and ultimately managing MS risk.
References
1. Latitudinal prevalence gradient of multiple sclerosis in Latin America. https://journals.sagepub.com/doi/full/10.1177/1352458511405562
2. Identification of a Latitude Gradient in the Prevalence of Primary MS. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8345914/
3. Latitude continues to be associated with MS prevalence. https://jnnp.bmj.com/content/89/6/A21.1
4. Latitude and vitamin D influence disease course in multiple sclerosis. https://www.nature.com/articles/nrneurol.2016.181
5. Evidence for early-life environmental exposures influencing MS risk. https://pubmed.ncbi.nlm.nih.gov/33704407/
6. The genetic predisposition to MS in European populations and its link to latitude. https://pubmed.ncbi.nlm.nih.gov/21478203/
7. Impact of improved healthcare access on MS incidence in low-latitude regions (example: Bogotá). https://www.sciencedirect.com/science/article/pii/S0013935117316730
8. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. https://www.science.org/doi/10.1126/science.abj8222
9. Smoking and multiple sclerosis: A systematic review and meta-analysis. https://journals.sagepub.com/doi/10.1177/1352458518801727