


Oral GLP-1 Agonists Show Major Promise

Recently, a new wave of drugs has been developed that puts obesity and type 2 diabetes in a chokehold. GLP-1 receptor agonists like Ozempic and Wegovy have transformed the treatment landscape for the two diseases, and possibly others. Originally developed to regulate blood sugar, they gained widespread attention for their ability to improve glycemic control as well as their ability to help with weight loss. Studies like the STEP 5 trial showed that semaglutide can lead to sustained weight loss exceeding 15% of body weight1. The strength of these results and their implications for public health and health expenditures related to the downstream effects of obesity and type 2 diabetes make them indispensable in the fight against these diseases. As promising as the results are, they have sparked debate about the role of medication vs lifestyle interventions.
In that vein, some critics have dismissed these drugs as the “easy way out” and solely promote exercise and diet while demonizing GLP-1 drugs. I find this oversimplification of the challenges faced by different individuals to be extremely unhelpful. Of course, doing all three in many cases of severe obesity or diabetes would obviously work the best and be the most health promoting action. But for those without the time or even the desire to exercise or eat healthier, an option to mitigate the effects of their lifestyle on obesity and type 2 diabetes should be available to them. While these medications have shown remarkable benefits, the most significant downside reported is a small reduction in lean muscle mass. Fortunately, this can be largely mitigated through targeted exercise programs aimed at building muscle, making the drugs even more effective when combined with physical activity. Imagine if a drug somehow made tobacco smoke non-carcinogenic or completely reversed the effects. I would like to think people would stand behind that drug and not demonize its use by smokers. With that said, despite their success in trials and as a prescribable drug, a significant barrier to its adoption does remain beyond anti-pharmaceutical sentiment: the delivery method. Plenty of people are put off by the idea of regular injections, even if they are with a user-friendly pen that is meant to be less painful. I imagine it being an injectable also comes with a bit of a stigma that deters adoption by some that a pill would not confer.
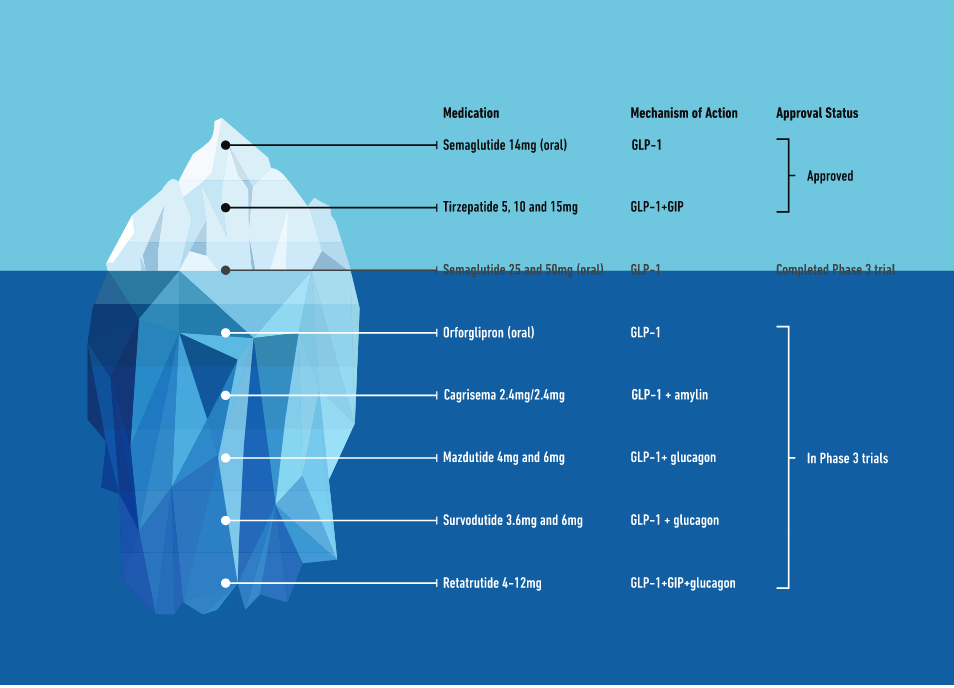
Now we have an exciting new frontier emerging in the advent of oral GLP-1 drugs. Here I will focus on Eli Lilly’s new drug Orforglipron (OFP) and a few other oral semaglutide medications. OFP is an oral, nonpeptide GLP-1 receptor agonist is currently under phase III clinical investigation and has shown promising results in its phase II results. The drug promises to address the hurdles of injectables while maintaining the significant benefits of prior drugs in the category. We could be entering a new era of metabolic care that radically redefines accessibility and adherence.
A (Very) Quick Look at What GLP-1 Drugs do and how they Work
GLP-1 receptor agonists mimic a natural hormone we have in the gut that helps to regulate blood sugar by enhancing insulin secretion, reducing glucagon, and slowing digestion. Essentially, these drugs help individuals to feel less hungry, thus reducing caloric intake. Beyond their effectiveness in diabetes and obesity, the drugs may also lower cardiovascular disease risk and help to address other obesity-related conditions 2.
Transitioning to Oral Options
The introduction of oral formulations of GLP-1 agonists marked a significant turning point for these therapies. The first oral GLP-1 drug was an oral formulation of semagulutide and was approved by the FDA in 2019 after trials showed efficacy in the PIONEER program. At the standard 14mg dose, it reduced HbA1c levels by up to 1.4% and had a mean weight loss association of 4.4kg 3. At higher doses of 25 and 50mg, there were even greater reductions in HbA1c and weight loss of up to 10% of body weight. While impressive, the higher doses also had higher rates of adverse events, particularly the gastrointestinal distresses that come with many GLP-1 drugs. The oral semaglutide also requires rather specific dosing conditions like taking the pill on an empty stomach and with water. More requirements for a drug typically means lower adherence, so a drug that can get around these issues would be more than welcome.
Some oral GLP-1 drugs have halted trials due to extensive adverse effects. A trial looking at Lotiglipron, another oral non-peptide GLP-1 drug was stopped in early phase trials due to the drugs association with elevated transaminases and concerns about liver toxicity. Another drug, danuglipron, will be unable to advance to phase 3 studies at the same dosage in phase II studies due to it having high rates of discontinuation due to adverse events, with 34% of participants stopping their use of the drug in trials4.
Emerging therapies like Orfoglipron are doing their best to address these limiting factors. Unlike oral semaglutide, OFP does not require food or water restrictions, further simplifying the administration process. Phase II trials showed decreases in HbA1c up to 2.1% compared to 0.43% in the placebo group3. Mean body weight decreased by 9.6% on OFP compared to 2.2% with placebo. Phase III trials are ongoing to extensively assess the safety and efficacy of the drug for both obesity and type 2 diabetes (Phase III Trial: NCT05872620). A bonus for OFP is the fact that it is considered a small-molecule design which may offer advantages in terms of scalability to potentially meet the growing demand for this class of drugs.
Transforming Metabolic Care
The future of oral GLP-1 drugs has massive promise in simplifying treatment programs and changing metabolic care. Combination therapies that integrate GLP-1 drugs with complementary mechanisms like amylin or glucagon co-agonists could enhance the weight loss and glycemic control while addressing broader metabolic challenges. This is already making waves in the injectables scene with treatments like Tirezepatide. Hopefully the oral counterparts look as solid as Orfoglipron is in early studies.
Beyond diabetes and obesity, GLP-1 drugs are being looked at for cardiovascular protection, liver health, cognitive disorders, and more. The range of applications is remarkable, but requires much more investigation. To fulfill their potential, scalability and affordability will need to be at the forefront to ensure the innovations are accessible to those most in need. The advancements in this space will be worth watching, and I’m certainly excited to keep an eye on things!
Citations and Further Reading
1. Lilly E. A Study of Daily Oral Orforglipron (LY3502970) Compared With Insulin Glargine in Participants With Type 2 Diabetes and Obesity or Overweight at Increased Cardiovascular Risk (ACHIEVE-4). Lilly Trials. Accessed January 1, 2025. https://trials.lilly.com/en-US/trial/397395
2. Lilly’s phase 2 results published in the New England Journal of Medicine show orforglipron, a once-daily oral nonpeptide GLP-1 receptor agonist, achieved up to 14.7% mean weight reduction at 36 weeks in adults with obesity or overweight | Eli Lilly and Company. Accessed January 1, 2025. https://investor.lilly.com/news-releases/news-release-details/lillys-phase-2-results-published-new-england-journal-medicine
3. Pfizer Announces Topline Phase 2b Results of Oral GLP-1R Agonist, Danuglipron, in Adults with Obesity | Pfizer. Accessed January 1, 2025. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-topline-phase-2b-results-oral-glp-1r
4. Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022;28(10):2083-2091. doi:10.1038/s41591-022-02026-4
5. Saxena AR, Frias JP, Brown LS, et al. Efficacy and Safety of Oral Small Molecule Glucagon-Like Peptide 1 Receptor Agonist Danuglipron for Glycemic Control Among Patients With Type 2 Diabetes: A Randomized Clinical Trial. JAMA Netw Open. 2023;6(5):e2314493-e2314493. doi:10.1001/jamanetworkopen.2023.14493
6. Wharton S, Blevins T, Connery L, et al. Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity. New England Journal of Medicine. 2023;389(10):877-888. doi:10.1056/NEJMoa2302392
7. Eli Lilly and Company. A Phase 3, Open-Label Study of Once Daily LY3502970 Compared With Insulin Glargine in Adult Participants With Type 2 Diabetes and Obesity or Overweight at Increased Cardiovascular Risk. clinicaltrials.gov; 2024. Accessed January 1, 2025. https://clinicaltrials.gov/study/NCT05803421
8. Friedman JM. The discovery and development of GLP-1 based drugs that have revolutionized the treatment of obesity. Proceedings of the National Academy of Sciences. 2024;121(39):e2415550121. doi:10.1073/pnas.2415550121
9. Gogineni P, Melson E, Papamargaritis D, Davies M. Oral glucagon-like peptide-1 receptor agonists and combinations of entero-pancreatic hormones as treatments for adults with type 2 diabetes: where are we now? Expert Opinion on Pharmacotherapy. 2024;25(7):801-818. doi:10.1080/14656566.2024.2356254
10. Ryan DH, Lingvay I, Deanfield J, et al. Long-term weight loss effects of semaglutide in obesity without diabetes in the SELECT trial. Nat Med. 2024;30(7):2049-2057. doi:10.1038/s41591-024-02996-7